Assessment Tools and Workflow
The program objectives of the MD program are based on the CanMEDS competencies of medical expert, communicator, collaborator, health advocate, scholar, professional and leader. Since assessment in Phase 4 is based in the workplace (i.e. clinical setting), Entrustable Professional Activities (EPAs) are used to assess learner competency. Refer to the EPA page for detailed descriptors of each EPA.
Assessment Tools
Entrustment decisions for EPAs can be either ad hoc assessments in the workplace or summative assessments at the end of a rotation or clinical block. The primary assessment tools to capture and document these decisions are In-Training Assessment Reports (ITARs) and electronic clinic cards. Each discipline has selected EPAs to be assessed in their rotation as outlined in this EPA assessment table. However, if needed or requested, any EPA may be assessed in any rotation.
Clinic Cards
Clinic cards are used for ad hoc EPA assessment in the workplace. They are completed by preceptors (residents or faculty) working with the learner for the clinical encounter being assessed. Clinic cards are formative and reflect the entrustment of the learner for that specific task/EPAs in the context of the specific clinical encounter and day. The preceptor rates the amount of supervision needed while the learner completed the task (“I guided the student through much of this activity”, “I provided corrective coaching tips on critical points during/after activity”, “I confirm the activity was successfully completed by the student”). Clinic cards should capture coaching comments provided to the learner by the preceptor.
Clinic cards are completed electronically, see How to Complete Clinic eCards. Only one to four EPAs are assessed on one card.
In-Training Assessment Reports (ITARs)
ITARs are used for formative and summative EPA assessment decisions. Summative ITARs are completed at the end of a rotation or clinical block by the primary preceptor and may encompass all EPAs (or additional ones) for the rotation. Preceptors assess the readiness of the leaner for entrustment of each of the included EPAs (“pre-entrustable”, “entrustable”). They also include written feedback for the learner.
The Clinical Discipline Coordinator (CDC) makes the final summative entrustment decision and documents this in the final ITAR for the rotation. The summative entrustment decision is primarily based on summative ITARs by preceptors but may be informed by other assessment tools and multiple ad hoc assessments (i.e. clinic cards). The final ITAR also summarizes learner performance for the Mini-CEX, discipline specific assessments and identifies any professionalism concerns.
Other assessment tools
The Mini-clinical evaluation exercise (mini-CEX) is used to assess a learner performing a witnessed history and physical. The preceptors observes the learner taking a history and completing a physical exam and scores their performance using a rubric. The Mini-CEX takes about 15 minutes to complete.
For any rotation longer than four weeks, learners receive mid-point feedback by the CDC during a scheduled meeting about half way through the rotation. This allows learners to review their performance, ensures they are on track to complete the required clinical experiences and procedures for that specific rotation and allows for mitigation of any issues and concerns.
Most disciplines also require learners to complete formative and summative discipline-specific assessments. A variety of different assessment methods are used for this purpose such as written assignments, completion of case studies, presentations or MCQ examinations.
Progress testing in the form of MCQ examinations is used to assess clinical knowledge. See here for more information.
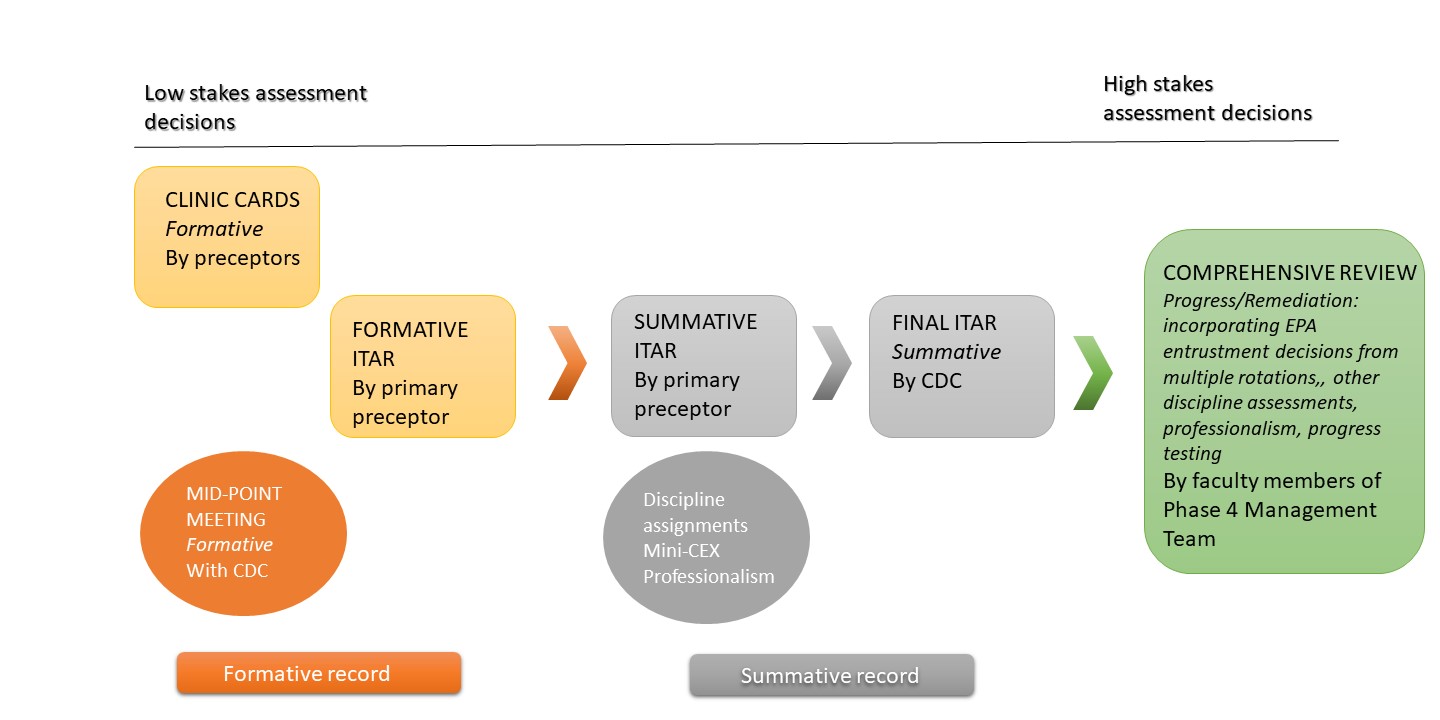
Assessment Workflow